
இந்தியாவின் பின்தங்கிய மாநிலத்தில் குழந்தைகள் ஊட்டச்சத்து குறைப்பாட்டை வெற்றிகரமாக குறைத்த சிறப்பு திட்டம்

பொகாரோ, ஜார்க்கண்ட்: இளம் செவிலியர் தாயான 25 வயது பூர்ணிமா தேவி, 25, தனது 21 மாத ஆண் குழந்தை கோரங்கோ மாலகருடன், 2018 ஆகஸ்ட் 11ஆம் தேதி ஜார்க்கண்டின் பொகாரோவில் உள்ள ஊட்டச்சத்து சிகிச்சை மையத்திற்கு (MTC) வந்தார். வெறும் 4.8 கிலோ எடையுள்ள இக்குழந்தை கடும் ஊட்டச்சத்து குறைபாட்டை கொண்டிருக்கும் வகையில் “சிவப்பு மண்டலம்” வகைப்பாட்டில் உள்ளது.
எடைகுறைபாடு, உடல் மெலிதல் போன்ற ஊட்டச்சத்து பற்றாக்குறையால் பாதிக்கப்பட்டுள்ள முதல் ஐந்து இந்திய மாநிலங்களில் ஜார்க்கண்ட்டும் ஒன்று என, சுகாதார மற்றும் குடும்ப நலத்துறை அமைச்சகத்தின் தேசிய குடும்ப சுகாதார ஆய்வறிக்கை 2015-16 -என்.எப்.எச்.எஸ். (NFHS-4) விவரத்தை இந்தியா ஸ்பெண்ட் பகுப்பாய்வு செய்ததில் தெரிய வந்துள்ளது. ஜார்க்கண்டில் ஐந்து வயதுக்குட்பட்ட குழந்தைகளில் ஏறத்தாழ பாதி பேர் (45.3%) வளர்ச்சி குன்றியவர்கள்; இதில் தேசிய சராசரி 38.4% ஆகும். குழந்தைகள் ஊட்டச்சத்து குறைப்பாட்டில் ஜார்க்கண்ட் மாநில குழந்தைகளில் பாதி பேர் (47.8%) எடை குறைபாடு உள்ளவர்கள்; இதில் பீகார், மத்தியப்பிரதேசத்திற்கு அடுத்ததாக இம்மாநிலம் உள்ளதை நமது பகுபாய்வுகள் காட்டுகின்றன. ஜார்கண்டில் குழந்தை இறப்பு விகிதம் 1,000 பிறப்புக்கு 44 மரணங்கள்; ஐந்து வயதுக்குட்ட குழந்தைகள் இறப்பு விகிதம் 1,000 பிறப்புக்கு 54 மரணங்கள் என்றுள்ளது; இதன் தேசிய சராசரி முறையே 41 மற்றும் 50 என, என்.எப்.எச்.எஸ். தெரிவிக்கிறது.
ஏழ்மை, பெண்கள் மத்தியில் அதிக கல்வியின்மை, இளம் வயது திருமணங்கள்,துப்புரவின்மை, ஊட்டச்சத்து விழிப்புணர்வு இல்லாமை, ஊட்டச்சத்து அணுகல் பற்றாக்குறை, போதிய உணவு இல்லாதது, வாழ்விடம், உள்ளூர் உணவு இழப்பு மற்றும் முறையான சுகாதாரப் பற்றாக்குறை உள்ளிட்டவை ஜார்கண்ட் மாநில குழந்தைகளின்ஊட்டச்சத்து குறைபாட்டுக்கு முக்கிய காரணங்கள். கனிம வளங்கள் நிறைந்திருந்தும் இந்தியாவில் அதிக வறுமை விகிதத்தை ஜார்க்கண்ட் கொண்டுள்ளது --3.3 கோடி மக்களில் 1.3 கோடி பேர் வறுமைக்கோட்டுக்கு கீழே வசிப்பதாக, உலக வங்கி சுயவிவரம் தெரிவிக்கிறது.
ஜார்க்கண்ட் அரசு ஓராண்டுக்கு முன், அரசுசாரா அமைப்பு (NGO), வேர்ல்ட் விஷன் இந்தியா அமைப்புடன் இணைந்து ஒருங்கிணைந்த குழந்தை மேம்பாட்டுத் திட்டம்-ஐசிடிஎஸ் (ICDS) --மாநில அரசாங்கங்களால் செயல்படுத்தப்படும் மத்திய அரசு திட்டம்-- பொகாரோ மாவட்டத்தில் இரண்டு ஒன்றியங்களில் ஊட்டச்சத்து குறைபாடு போக்கும் திட்டங்களை தொடங்கியது. இந்தியா ஸ்பெண்ட் நேரடி கள ஆய்வில், இந்த சிறப்பு திட்டத்தில் வீட்டுக்கு வீடு சென்று குழந்தைகளை கண்காணித்தல், அங்கன்வாடி பணியாளர்களுக்கு பயிற்சி, நிலையான ஆதரவு மற்றும் திறம்பட கண்காணிப்பு ஆகியவற்றால் இரண்டு ஒன்றியங்களில் ஊட்டச்சத்து இல்லாத குழந்தைகளில் 61% பேர் குணப்படுத்தப்பட்டனர்.
ஊட்டச்சத்து குறைபாட்டுக்கு வறுமையே காரணம்; ஜார்க்கண்ட் கிராமப்புற குடும்பங்கள் சுகாதார வசதியை அணுக தடையாக உள்ள ஏழ்மை
சில மாதங்களில் இரண்டாம் முறையாக, பூர்ணிமாவின் குழந்தை மீண்டும் சிவப்பு நிற வகைப்பாட்டிற்குள் வந்தது. பொதுவாக குழந்தைகளின் ஊட்டச்சத்து குறைப்பாட்டை அவர்களின் கையில் நடுப்பகுதியின் மேல் சுற்றளவு -எம்.யு.ஏ.சி. (MUAC) அளவை கொண்டு கணக்கிடப்படுகிறது. நிலையான அளவு டேப் கொண்டு அளந்து இது பச்சை, மஞ்சள் சிவப்பு வகைப்பாட பிரிக்கப்படுகிறது. ஊட்டச்சத்து குறைப்பாட்டில், பச்சை நிற வகைப்பாடு என்பது எம்.யு.ஏ.சி. அளவு 12.5 செ.மீ. - 26 செ.மீ.க்கு இடைப்பட்டதாக இருக்கும். மஞ்சள் நிற வகைப்பாட்டில் 12.5 செ.மீ. - 11.5 செ.மீக்கு இடையிலும்; சிவப்பு நிற வகைப்பாட்டில் எம்.யு.ஏ.சி. அளவு 11.5 செ.மீ.க்கு குறைவாக இருக்கும்; இது கடும் ஊட்டச்சத்து குறைபாட்டையும், அவசர மருத்துவ பாதுகாப்பின் அவசியத்தையும் வெளிப்படுத்துவதாகும்.
பூர்ணிமாவின் குழந்தையுடைய கையின் நடுப்பகுதியை அளவிட்ட அங்கன்வாடி ஊழியர்கள், கோரங்கோவின் உடல்நிலை அபாயகட்டத்தில் இருப்பதாகக்கூறி, பொகாரோவில் உள்ள எம்.டி.சி. மையத்திற்கு அழைத்துச் செல்ல பரிந்துரை செய்தனர். பொகாரோவில் உள்ள எம்.டி.சி. மையம் 20 படுக்கைகளை கொண்டது; ஆனால் இந்தியா ஸ்பெண்ட் பார்வையிட்டபோது கோரங்கோ மட்டுமே நோயாளியாக சேர்க்கப்பட்டிருந்தது. எனினும், ஊட்டச்சத்து குறைபாடு குறைவாக உள்ளது என்பது இதன் பொருளல்ல.
எம்.சி.சி. மையத்திற்கு வரும் ஊட்டச்சத்து குறைபாடுள்ள குழந்தைகளின் பல பெற்றோர்களுக்கு அதுதான் கடைசி முடிவாக உள்ளது; ஏனெனில், குடும்பங்கள் தங்களுடைய தினசரி ஊதியத்தை இழக்க அஞ்சுகின்றன. பொகாரோ சுகாதார மையத்திற்கு பூர்ணிமா தேவி வருவதற்கு, ஜார்க்கண்ட்- மேற்கு வங்க எல்லையில் உள்ள தனது கிராமத்தில் இருந்து 10 கி.மீ. தொலைவு பயணம் செய்ய வேண்டியிருந்தது. மற்றவர்கள் மாவட்ட தலைமையகத்தை அடைய 40 கி.மீ.க்கு பயணம் செய்ய வேண்டும். “ஆகஸ்ட் மாதம் விதைப்பு பருவம் என்பதால் விவசாய தொழிலாளர்கள் தேவை அதிகமாக இருக்கும்” என்று, பொகாரோ எம்.டி.சி. பணியாளர் நிஷா சிங் தெரிவித்தார். “தங்கள் குழந்தைக்கு ஊட்டச்சத்து குறைபாடு இருப்பினும், இங்கு வருவதற்காக ஒருநாள் கூலியை விட்டுக்கொடுக்க பெற்றோர் விரும்புவதில்லை. அவர்கள், அருகில் உள்ள அங்கன்வாடி மையங்களுக்கு குழந்தையை கொண்டு செல்வர்; அல்லது வீட்டிலேயே சிகிச்சை அளித்து தோல்வி காண்பார்கள்” என்றார்.
கிழக்கு பொகரோ மாவட்டம் சந்தங்கிரி ஒன்றியம் தெக்கோரா கிராமத்தில் உள்ள அங்கன்வாடி தொழிலாளர் சாயா முகர்ஜி இந்தியா ஸ்பெண்டிடம் கூறுகையில் அங்கன்வாடி மையத்தில் தான் பணிபுரிந்த இரண்டரை ஆண்டுகளில், எம்டிசியில் குழந்தைகளை சேர்க்க தயங்கிய பல தாய்மார்களை கண்டதாக கூறினார். தனது பகுதியில் 3 குழந்தைகள் கடும் ஊட்டச்சத்து பற்றாக்குறையால் அவதிப்பட்ட நிலையில் ஒரு குழந்தை மட்டுமே எம்.டி.சி.யில் அனுமதிக்கப்பட்டிருந்ததாக அவர் தெரிவித்தார். "ஒருசில தாய்மார்கள் ஊட்டச்சத்து குறைபாடுகளை புரிந்து கொள்ளத்தவறிவிட்டார்கள், பலரும் வேலைகளை விட்டு வர முடியாது," என்றார் முகர்ஜி.
ஒரு சந்தர்ப்பத்தில், 25 வயதான கொஸாம்தேவி தனது ஒன்பது மாத குழந்தையை எம்.டி.சி.க்கு கொண்டு வந்தார். அக்குழந்தை ஒருமுறை மட்டுமே உற்சாகமடைந்தது. "குழந்தையின் நிலை பற்றி முன்பே நாங்கள் எச்சரிக்கை செய்தோம்; ஆனால் அவர் தனது கிராமத்தில் இருந்து 50 கி.மீ. தொலைவில் உள்ள எம்.டி.சி.க்கு வரவில்லை; போக்குவரத்திற்கு அவரிடம் பணம் இல்லை" என்று முகர்ஜி தெரிவித்தார்.

கொஸும் தேவி (நடுவில் இருப்பவர்) தனது கணவர் (இடது) மற்றும் ஒன்பது மாத ஊட்டச்சத்து குறைபாடுள்ள குழந்தையுடன். அருகில், பொகாரோ ஊட்டச்சத்து சிகிச்சை மையத்திற்கு அவர்களை அழைத்து வந்த அங்கன்வாடி பணியாளர்.
"தாய்மார்கள் தினந்தோறும் கூலி வேலைக்கு செல்வதானால், ஒவ்வொரு ரூபாயும் அவர்கள் கணக்கிடுகிறார்கள்," பூர்ணிமா கூறினார். "எம்.டி.சி. சார்பில் குழந்தையின் உதவியாளருக்கு நாளொன்றுக்கு 100 ரூபாய் இழப்பீடு தரப்படுகிறது; ஆனால், உணவுக்கு மட்டும் தான் போதுமானது. வேலைக்கு செல்லாமல் குழந்தையை பார்த்து கொண்டிருந்தால், அவர்கள் குடும்பத்தில் மற்றவர்கள் எப்படி வாழ்வார்கள்?” என்று அவர் கேட்டார்.
பூர்ணிமாவின் இக்கட்டான சூழ்நிலைக்கு வறுமை என்பது அடிப்படை காரணம். ஊட்டச்சத்து குறைபாட்டைத் தவிர்ப்பதற்காக, பாலூட்டும் ஒரு தாய் காய்கறிகள், நார் மற்றும் புரதம் நிறைந்த உணவுகளை சாப்பிட வேண்டும். ஆனால், மிஞ்சிய உணவுகளை தான் பூர்ணிமா சாப்பிடுகிறார். ”மற்ற பெண்களை போல தான் நானும் வீட்டில் கடைசியாக உணவு சாப்பிடுகிறேன். ஒரு நாளை இரண்டு முறை வேகவைத்த அரிசி, கொஞ்சம் பருப்பு என கிடைப்பதை சாப்பிடுகிறேன்” என்று இந்தியா ஸ்பெண்டிடம் பூர்ணிமா தெரிவித்தார். அவருக்கு ஊட்டம் நிறைந்த உணவு தேவை என்பதை குடும்பத்தினரும் அறிவார்கள்; எனினும் உணவை அதிகம் தர முடியாது. தண்ணீர் பிடிப்பது, குடும்பத்தில் உள்ள ஏழு பேருக்கு சமைப்பது மற்றும் அவர்களின் துணிகளை துவைப்பது என்று, பூர்ணிமாவின் தினசரி வாழ்க்கை நகர்கிறது; சுய பாதுகாப்பு குறித்து அவர் அக்கறை எடுத்துக் கொள்ள முடிவதில்லை.
ஜார்கண்ட் மாநிலத்தில் வறுமைக் கோட்டுக்கு கீழே உள்ள பெரும்பான்மையான பெண்களின் கதையும் பூர்ணிமாவை போன்றது தான். இங்குள்ள பல செவிலியர் தாய்மார்கள், ஒருநாளைக்கு இரண்டு வேளை உணவே உண்டு ஊட்டச்சத்து குறைவோடு உள்ளனர்; ஊட்டக்குறைபாடு உள்ள குழந்தைகள் பிறக்க இது வழிவகுக்கிறது.
கல்வியின்மை மற்றும் ஊட்டச்சத்து குறைபாடு ஆகியவற்றுக்கு இடையே நெருக்கமான இணைப்பு உள்ளது. இந்தியாவின் 2011 மக்கள் தொகை கணக்கெடுப்புபடி, ஜார்க்கண்டின் மக்கள்தொகையில் 76% கிராமப்புறங்களில் வாழ்கின்றனர்; இதில் இந்திய சராசரி 31% ஆகும். இந்திய கிராமப்புற பெண்களின் கல்வி விகிதம் 62% என்பதுடன் ஒப்பிடும்போது, ஜார்கண்ட் மாநில கிராமப்புற பெண்களில் 46.62% கல்வி பெற்றுள்ளனர். ஜார்க்கண்ட் கிராமப்புறங்களில் 15-49 வயதுடைய பெண்களில் 67.3%; ஆறு முதல் 59 வயதுடைய பெண்களில் 71.5% பேர் ரத்தசோகையால் பாதிக்கப்பட்டுள்ளனர். இதில் தேசிய சராசரி முறையே 53.1% மற்றும் 58.6% என்று உள்ளதாக என்.எப்.எச்.எஸ். புள்ளி விவரங்கள் தெரிவிக்கின்றன.
பல பெண்கள் 18 வயதிற்கு முன்பே திருமணம் செய்து கொண்டனர், 14 வயதிற்கு உட்பட்டவர்களாகவும், அவர்களுக்குக் கல்வி கற்றுக்கொடுப்பது குறைவாகவும் உள்ளது. ஜார்கண்ட் மாநிலத்தில் 37.9% பெண்கள் திருமணத்திற்கும் குறைவான வயதுடையவர். இது நாட்டின் மூன்றாவது உயர்ந்த விகிதமென என்.எப்.எச்.எஸ். தரவுகளை கொண்ட எமது பகுப்பாய்வு காட்டுகிறது. "எந்த வயதினரும் தங்கள் வயது என்ன என்று கேட்கும்போது 25 இருக்கும் என்று பதில் அளிக்கின்றனர்" என்று ஒரு அங்கன்வாடி ஊழியர் தெரிவித்தார். "குடும்ப உறுப்பினர்கள் தங்கள் பிறந்த தேதி பற்றி தெரியாது. ஆதார் அட்டையில் (மத்திய அரசின் தனித்துவ அடையாளம் காணும் திட்டம்) பதிவு செய்யும்போது, தாய்மார்கள் பலர் தங்கள் வயதை 18 என்றே குறிப்பிட்டுள்ளனர். 14 வயதான பெண்களை பள்ளியில் இருந்து நிறுத்தி திருமணம் செய்து வைக்கப்பட்டிருப்பதை தனிப்பட்ட முறையில் நான் கண்டேன்”. தனக்கு 25 வயது என்றும் ஆனால் பார்ப்பதற்கு இன்னும் இளையவராக தெரிவதாக, பூர்ணிமா தேவி கூட தெரிவித்தார்.
சுகாதார குறைபாடு நிலைமைகள் நோய்களின் பரவலுக்கு காரணமாகின்றன; இது ஊட்டச்சத்துக் குறைபாட்டின் மற்றொரு முக்கிய காரணம். ஜார்க்கண்ட் கிராமங்களில் குடிநீர் என்பது சுத்தமற்றது; பெரும்பாலும் பாசி நிறைந்த குளங்களில் இருந்து குடிநீர் பெறப்படுகிறது.
ஊழியர்கள், ஆதார வளங்களால் ஊட்டச்சத்து குறைபாட்டுக்கு எதிரான போராட்டத்தில் முன்னிலை வகிக்கும் ஜார்கண்ட் அங்கன்வாடி மையங்கள்
கடந்த 1990ஆம் ஆண்டுகளில் இருந்து ஊட்டச்சத்து குறைபாடு தொடர்பான பாதிப்புகள் இந்தியாவில் குறைந்து வருகிறது. 2016ஆம் ஆண்டில் இந்தியாவின் மொத்த நோய் பாதிப்பில் ஊட்டச்சத்து குறைப்பாட்டின் பங்கு 15% என்றளவில் இருந்தது என, “இந்தியா: ஹெல்த் ஆப் தி நேஷன்’ஸ் ஸ்டேட்டஸ்” இந்தியாவின் மாநில அளவிலான நோய்கள் சுமை குறித்த முன்முயற்சியின் அறிக்கையில் தெரிவிக்கப்பட்டுள்ளது.
தேசிய அளவில் பத்து ஆண்டுகளுக்கு முன் ஒப்பிடும் போது, 2015-16ஆம் ஆண்டில் குழந்தைகள் ஊட்டச்சத்து குறைபாடு 9.6% புள்ளி குறைந்துள்ளது. ஆனால் ஜார்கண்டின் முன்னேற்ற விகிதம், 4.5% என என்.எப்.எச்.எஸ். தரவின் எங்கள் பகுப்பாய்வு காட்டுகிறது.
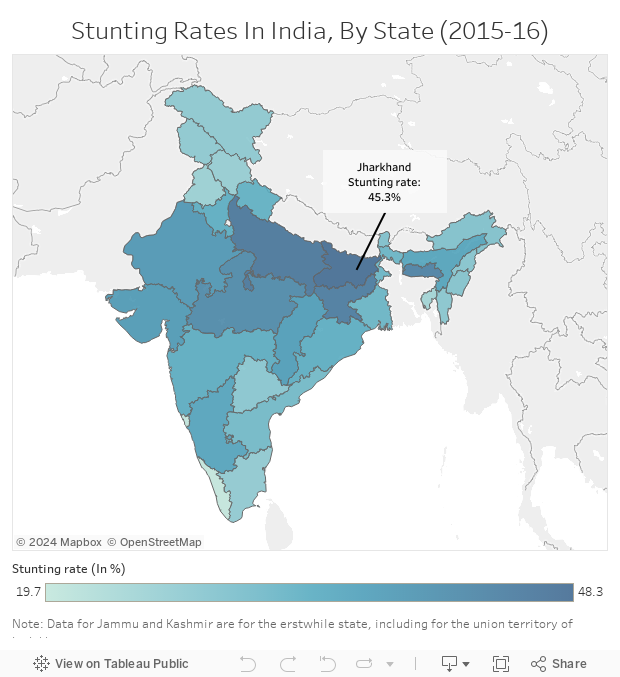
Source: National Family Health Survey 4 (2015-16)
கடந்த 2017, நவம்பர் 21ல் ஜார்கண்ட் முதலமைச்சர் ரகுபார் தாஸ் ஓர் அறிவிப்பை வெளியிட்டார். அதன்படி, ஊட்டச்சத்து குறைபாட்டை குறைக்கும் வகையில், 2018ஆம் ஆண்டு ‘நிரோக் பால் வர்ஷ்’ ( ஆரோக்கிய குழந்தைக்கான ஆண்டு) என கடைபிடிக்கப்படும் என்று அறிவிக்கப்பட்டது. “அடுத்த மூன்று, நான்கு ஆண்டில் ஊட்டச்சத்து மிகுந்த மாநிலங்களில் முதல் 10 இடங்களுக்குள் வருவதே ஜார்க்கண்டில் இலக்கு” என்று தாஸ் தெரிவித்தார்.
எனினும், அந்த இலக்கை அடைய ஜார்க்கண்ட்டிற்கு ஒரு நீண்ட நெடிய பயணமாக உள்ளது. 2018 ஆகஸ்ட் 19ல், தலைநகர் ராஞ்சியில் உள்ள சர்தார் மருத்துவமனையில் ஒரு குழந்தை, தனியார் மருத்துவமனையில் மற்றொரு குழந்தை உயிரிழந்தது. ஒரு வாரத்திற்குள்ளாக ஆகஸ்ட் 24ஆம் தேதி, தாயால் கைவிடப்பட்ட ஒரு ஆண் குழந்தை, ராஞ்சி ராஜேந்திரா மருத்துவ அறிவியல் கழக மருத்துவமனையில் இறந்தது. இம்மூன்று குழந்தைகளுமே எடை குறைபாடு, ஊட்டச்சத்துயின்மையால் இறந்தன.
ஜார்கண்ட் மாநிலத்தில் ஊட்டச்சத்து குறைபாடுள்ள குழந்தைகளின் எண்ணிக்கை அதிகம் இருப்பது, ஊட்டச்சத்து திட்டங்களின் செயல்திறனை கேள்விக்குறியாக்குகிறது. மாநில சமூக நலத்துறையால் நடத்தப்படும் அங்கன்வாடி மையங்கள், பெரும்பாலான குழந்தைகளுக்கு அணுகல் இடமான ஐ.சி.டி.எஸ். போன்றவற்றில் போதிய ஊழியர், ஆதாரவளங்கள் இல்லாததுடன் போராட வேண்டியுள்ளது.
பெயர் வெளியிட விரும்பாத, பொகாரோ மாவட்ட அங்கன்வாடி மைய மேற்பார்வையாளர் இந்தியா ஸ்பெண்டிடம் கூறுகையில், பணியாளர் பற்றாக்குறை இதற்கான காரணம் என்றார். ”பொகாரோ மாவட்டத்தில் 324 அங்கன்வாடி மையங்கள் உள்ளன; ஆனால், எதிலும் முழுமையான வசதிகள் இல்லை” என மேற்பார்வையாளர் தெரிவித்தார். “ஒவ்வொரு அங்கன்வாடி ஊழியரும் குறைந்தது 35 மையங்களுக்கு பொறுப்பாக உள்ளார். ஒவ்வொன்றும் வெகுதூரத்தில் உள்ளது; அவற்றை சென்றடைய சாலை (பாதை) வசதியில்லை என்பதால், சேவை புரிவது கடினமாக உள்ளது” என்றார். மோசமான, வெளிச்சமற்ற பொகாரோ கிராமப்புற சாலைகள் நிலைமையை மேலும் மோசமாக்குகிறது. பொகாரோ எம்.டி.சி. வருவதற்கு 6 கி.மீட்டருக்கு மேல் நடந்து, இரண்டு பேருந்துகளை பிடிக்க வேண்டும் என்று, பூர்ணிமா தேவி தெரிவித்தார்.
"பொகரோவிலிருந்து தெக்கோரா கிராமத்திற்கு 22 கி.மீ. தொலைவில் காடுகள், சாலைகளில் நாங்கள் பயணம் செய்ய வேண்டும். கிராமங்களுக்கு இடையே சென்று வருவதற்குள் சோர்வு ஏற்பட்டுவிடுகிறது” என, சந்தன்கியரி ஒன்றிய அங்கன்வாடி மேற்பார்வையாளர் ரூபா குமாரி தெரிவித்தார். “ஆனால், எங்களுக்கு இது கொஞ்சம் தான்; நிறைய குழந்தைகள் அவசர உதவி தேவையோடு இருக்கிறார்கள்; அவர்களுக்கு உதவ நாங்கள் விரும்புகிறோம்” என்றார் ரூபா.
கடந்த இரண்டு ஆண்டுகளாக மாநில அரசு பயணப்படியை வழங்காத நிலையில் மேற்பார்வையாளர்கள் தங்களின் சொந்த பணத்தில் கிராமங்களுக்கு சென்று வருவதாக, ஒரு மேற்பார்வையாளர் தெரிவித்தார். எம்.டி.சி., அல்லது மாவட்ட தலைமையகத்தில் குழந்தைகள் அல்லது மேற்பார்வையாளர்களுக்கு உதவுவதற்காக வாகனங்கள் இல்லை.
சிக்கலான நிலையில் எம்.டி.சி.யில் விடப்படும் குழந்தைகள், ஊட்டச்சத்து குறைபாடு உள்ள தாய்மார்கள், குழந்தைகள் போதிய ஊட்டம் பெறச் செய்தல் என்று அங்கன்வாடி ஊழியர்களுக்கு பணிச்சுமை அதிகளவில் உள்ளது. ஒரு ஊட்டச்சத்து குறைபாடுள்ள குழந்தை மருந்திற்காக குறைந்தபட்சம் 15 நாட்களுக்கு எம்.டி.சி.யில் மருந்து மற்றும் கண்காணிப்புக்காக அனுமதிக்கப்பட வேண்டும்; ஆனால் பெரும்பாலான பெற்றோர்கள் இரண்டு நாட்களுக்கு மேல் தங்க மறுக்கிறார்கள்; அவர்கள் தினசரி சம்பளம் இழந்துவிடும் என்ற அச்சமே காரணம். அங்கன்வாடி ஊழியர்களின் பொறுப்புகள், 15 நாட்களுக்கு தங்குவதற்கு குடும்பத்தினருக்கு ஆலோசனை வழங்குவதும் அடங்கும். இத்தகைய ஆலோசனைக்கு வழங்கும் ஊழியர்களுக்கு கடும் பற்றாக்குறை உள்ளதன் விளைவுகள், அவர்கள் முழு 15 நாள் சிகிச்சைக்கு செல்லவில்லை என்றால் ஊட்டச்சத்து நிறைந்த குழந்தைகள் உருவாவதை அதிகரிக்கிறது.
ஜார்க்கண்ட் மாநிலத்தில் தேசிய ஊரக சுகாதார திட்டத்தை செயல்படுத்தும் மத்திய சுகாதார மற்றும் குடும்ப நலத்துறை இயக்குனர் கிருபானந்த் ஜா, ஊட்டச்சத்து குறைப்பதற்கான நடவடிக்கைகளை துரிதப்படுத்துவதாக கூறுகிறார். “ஜார்க்கண்ட் மாநிலத்தில் 88 சதவீத குழந்தைகளுக்கு சிகிச்சை தரப்பட்டுள்ளது; 75 சதவீதம் வாய்வழியே உப்பு கரைசல் தரப்பட்டுள்ளது” என்று ஜா தெரிவித்தார்.
மாநிலத்தின் குழந்தைகளுக்கான ஊட்டச்சத்து நெருக்கடியை சமாளிக்கும் வகையில் மருந்து வினியோகம் மீதான கவனம் போதுமானதாக இல்லை. ஐ.சி.டி.எஸ் மற்றும் அங்கன்வாடி மையங்களை நன்கு பராமரிப்பது மற்றும் குழந்தை ஊட்டச்சத்து குறைபாடுகளை அங்கன்வாடி பணியாளர்கள் சமாளிப்பது மிகவும் திறமையான அணுகுமுறையாக இருக்க முடியும் என்று இந்த சிறப்பு திட்டம் காட்டுகிறது.
பொகரோவின் ஊட்டச்சத்து மேலாண்மை சிறப்பு திட்டம் ஜார்கண்டிற்கு வழி காட்டுகிறது
பொகாரோ மாவட்டத்தின் சந்தன்கியாரி மற்றும் சாஸ் ஒன்றியங்களில், 2017 ஜனவரி- செப்டம்பர் இடையே ஒன்பது மாதங்கள் செயல்படுத்தப்பட்ட ‘சமுதாய அடிப்படையிலான தீவிர ஊட்டச்சத்து மேலாண்மை’ (CMAM) சிறப்பு திட்டம், குழந்தைகளின் ஊட்டச்சத்து குறைபாடுகளை குறைக்க பெரிதும் உதவியது. ஜார்க்கண்ட் மாநில ஊட்டச்சத்து இயக்கம், அரசுசாரா அமைப்பான வேர்ல்ட் விஷன் இந்தியா (WV India) உடன் சேர்ந்து இந்தியா முழுவதும் சுகாதார வசதிகளை மேம்படுத்துதல், ஆதரவு மேற்பார்வை மற்றும் திறனை வளர்ப்பதில் அனுபவத்தை கொண்டு, இத்திட்டத்தை செயல்படுத்தியது.
இத்திட்டத்தில் வீடுவீடாக சென்று குழந்தைகள் கண்காணிக்கப்பட்டனர்; அவர்களது கையின் நடுப்பகுதி சுற்றளவு அளவிடப்பட்டது. டபிள்யூ.வி. இந்தியா அங்கன்வாடி ஊழியர்களுக்கு பயிற்சி அளித்ததோடு தன்னார்வலர்களை கொண்டு பயிற்சியை கண்காணித்தது. இந்த திட்டம், மஞ்சள் மற்றும் சிவப்பு நிற வகைப்பாடு அடையாளம் கொண்ட குழந்தைகளுக்கு, அதாவது முறையே மிதமான ஊட்டச்சத்து பற்றாக்குறை நிலை மற்றும் தீவிர ஊட்டச்சத்து பற்றாக்குறை நிலை என்ற பிரிவில் சிகிச்சை அளிப்பதை மையமாகக் கொண்டது.
இதன் முடிவுகள், மஞ்சள் நிற வகைப்பாட்டில் இருந்த 158 குழந்தைகளில் 96 பேர் (61%) ஊட்டச்சத்து குறைபாட்டில் இருந்து மீண்டனர். சிவப்பு நிற வகைப்பாடு குழந்தைகள் உடனடியாக எம்.டி.சி.களுக்கு அனுப்பப்பட்டனர்.
"டபிள்யூ.வி. இந்தியாவின் ஈடுபாட்டிற்கு முன்னர் ஊட்டச்சத்து குறைபாடுகளின் எண்ணிக்கை குறைவாக இருந்தது" என, அதன் தொழில்நுட்ப வல்லுனரான கிரானாபுல் செல்வி இந்தியா ஸ்பெண்டிடம் தெரிவித்தார். "ஆதார வளங்களும், நேரமும் இல்லாததால், களத்தில் உள்ள அரசு ஊழியர்கள் ஊட்டச்சத்துள்ள குழந்தைகளை அடையாளம் காண முடியவில்லை. உண்மை கள நிலவரம் வேறு மாதிரியாக இருப்பினும், மூத்த அதிகாரிகள் நம்பிக்கையூட்டும் வகையில் சித்தரித்தனர்” என்றார்.
டபிள்யு.வி. இந்தியாவின் உறுதியான நிறுவன ஆதரவு, மருந்து வழங்கலை உறுதி செய்தது; சத்தான உணவு, குழந்தைகளின் துல்லியமான நிலை குறித்து ஆய்வறிக்கை தந்தது என செல்வி கூறினார். ஐ.சி.டி.எஸ். செயலாக்கத்திற்கான மாநில அரசுடன் இந்த குறுகிய கால ஒத்துழைப்பு சாதகமான முடிவுகளை வழங்கியது என அவர் மேலும் கூறினார்.

பொகாரோ மாவட்டத்தில் உள்ள அங்கன்வாடி மையம் ஒன்றின் சுவற்றில் ஊட்டச்சத்து மிகுந்த உணவு குறித்து மக்களுக்கு விழிப்புணர்வு ஏற்படுத்தும் விளம்பரம் இடம் பெற்றுள்ளது.
சி.எம்.ஏ.எம். திட்டம், பிரச்சனைகளை ஒரு வரம்புக்குள் நிர்வகிக்க உதவியது என்று மாநில சமூகநல துறை தலைவர் சுமன் குப்தா, பொகாராவில் இந்தியா ஸ்பெண்டிடம் தெரிவித்தார். "இது ஊட்டச்சத்து குறைபாட்டின் மோசமான சூழ்நிலையை புரிந்துகொள்ள உதவியது; இதன்மூலம் குழந்தைகள் உடனடியாக பராமரிக்கப்பட்டனர். அரசால் வளங்களை நன்கு நிர்வகிக்க முடிந்தது” என்று குப்தா தெரிவித்தார்.
"தாய்மார்களுடன் தொடர்பு கொள்வதற்கான வழிகளை வேர்ல்ட் விஷன் கற்பிப்பதன் மூலம் எங்கள் தொழில்முறை திறன்களை அதிகரிக்கிறது. நாங்கள் தாய்மார்களிடம் சுகாதார மற்றும் சுய பராமரிப்பு கவனத்தை கொஞ்சம் கொஞ்சமாக செலுத்த முடியும். அதுவே முன்னேற்றம் தான், "என்கிறார் ஒரு அங்கன்வாடி பணியாளர்.
(இந்த கட்டுரை குழந்தை சுகாதார, கல்வி மற்றும் குழந்தை பாதுகாப்பு குறித்த டபிள்யு.வி.ஐ. - எல்.டி.வி.(WVI- LDV) உடன் இணைந்த ஒரு பகுதியாக உள்ளது.)
உங்களின் கருத்துகளை வரவேற்கிறோம். கருத்துகளை respond@indiaspend.org. என்ற முகவரிக்கு அனுப்பலாம். மொழி, இலக்கணம் கருதி அவற்றை திருத்தும் உரிமை எங்களுக்கு உண்டு.
பொகாரோ, ஜார்க்கண்ட்: இளம் செவிலியர் தாயான 25 வயது பூர்ணிமா தேவி, 25, தனது 21 மாத ஆண் குழந்தை கோரங்கோ மாலகருடன், 2018 ஆகஸ்ட் 11ஆம் தேதி ஜார்க்கண்டின் பொகாரோவில் உள்ள ஊட்டச்சத்து சிகிச்சை மையத்திற்கு (MTC) வந்தார். வெறும் 4.8 கிலோ எடையுள்ள இக்குழந்தை கடும் ஊட்டச்சத்து குறைபாட்டை கொண்டிருக்கும் வகையில் “சிவப்பு மண்டலம்” வகைப்பாட்டில் உள்ளது.
எடைகுறைபாடு, உடல் மெலிதல் போன்ற ஊட்டச்சத்து பற்றாக்குறையால் பாதிக்கப்பட்டுள்ள முதல் ஐந்து இந்திய மாநிலங்களில் ஜார்க்கண்ட்டும் ஒன்று என, சுகாதார மற்றும் குடும்ப நலத்துறை அமைச்சகத்தின் தேசிய குடும்ப சுகாதார ஆய்வறிக்கை 2015-16 -என்.எப்.எச்.எஸ். (NFHS-4) விவரத்தை இந்தியா ஸ்பெண்ட் பகுப்பாய்வு செய்ததில் தெரிய வந்துள்ளது. ஜார்க்கண்டில் ஐந்து வயதுக்குட்பட்ட குழந்தைகளில் ஏறத்தாழ பாதி பேர் (45.3%) வளர்ச்சி குன்றியவர்கள்; இதில் தேசிய சராசரி 38.4% ஆகும். குழந்தைகள் ஊட்டச்சத்து குறைப்பாட்டில் ஜார்க்கண்ட் மாநில குழந்தைகளில் பாதி பேர் (47.8%) எடை குறைபாடு உள்ளவர்கள்; இதில் பீகார், மத்தியப்பிரதேசத்திற்கு அடுத்ததாக இம்மாநிலம் உள்ளதை நமது பகுபாய்வுகள் காட்டுகின்றன. ஜார்கண்டில் குழந்தை இறப்பு விகிதம் 1,000 பிறப்புக்கு 44 மரணங்கள்; ஐந்து வயதுக்குட்ட குழந்தைகள் இறப்பு விகிதம் 1,000 பிறப்புக்கு 54 மரணங்கள் என்றுள்ளது; இதன் தேசிய சராசரி முறையே 41 மற்றும் 50 என, என்.எப்.எச்.எஸ். தெரிவிக்கிறது.
ஏழ்மை, பெண்கள் மத்தியில் அதிக கல்வியின்மை, இளம் வயது திருமணங்கள்,துப்புரவின்மை, ஊட்டச்சத்து விழிப்புணர்வு இல்லாமை, ஊட்டச்சத்து அணுகல் பற்றாக்குறை, போதிய உணவு இல்லாதது, வாழ்விடம், உள்ளூர் உணவு இழப்பு மற்றும் முறையான சுகாதாரப் பற்றாக்குறை உள்ளிட்டவை ஜார்கண்ட் மாநில குழந்தைகளின்ஊட்டச்சத்து குறைபாட்டுக்கு முக்கிய காரணங்கள். கனிம வளங்கள் நிறைந்திருந்தும் இந்தியாவில் அதிக வறுமை விகிதத்தை ஜார்க்கண்ட் கொண்டுள்ளது --3.3 கோடி மக்களில் 1.3 கோடி பேர் வறுமைக்கோட்டுக்கு கீழே வசிப்பதாக, உலக வங்கி சுயவிவரம் தெரிவிக்கிறது.
ஜார்க்கண்ட் அரசு ஓராண்டுக்கு முன், அரசுசாரா அமைப்பு (NGO), வேர்ல்ட் விஷன் இந்தியா அமைப்புடன் இணைந்து ஒருங்கிணைந்த குழந்தை மேம்பாட்டுத் திட்டம்-ஐசிடிஎஸ் (ICDS) --மாநில அரசாங்கங்களால் செயல்படுத்தப்படும் மத்திய அரசு திட்டம்-- பொகாரோ மாவட்டத்தில் இரண்டு ஒன்றியங்களில் ஊட்டச்சத்து குறைபாடு போக்கும் திட்டங்களை தொடங்கியது. இந்தியா ஸ்பெண்ட் நேரடி கள ஆய்வில், இந்த சிறப்பு திட்டத்தில் வீட்டுக்கு வீடு சென்று குழந்தைகளை கண்காணித்தல், அங்கன்வாடி பணியாளர்களுக்கு பயிற்சி, நிலையான ஆதரவு மற்றும் திறம்பட கண்காணிப்பு ஆகியவற்றால் இரண்டு ஒன்றியங்களில் ஊட்டச்சத்து இல்லாத குழந்தைகளில் 61% பேர் குணப்படுத்தப்பட்டனர்.
ஊட்டச்சத்து குறைபாட்டுக்கு வறுமையே காரணம்; ஜார்க்கண்ட் கிராமப்புற குடும்பங்கள் சுகாதார வசதியை அணுக தடையாக உள்ள ஏழ்மை
சில மாதங்களில் இரண்டாம் முறையாக, பூர்ணிமாவின் குழந்தை மீண்டும் சிவப்பு நிற வகைப்பாட்டிற்குள் வந்தது. பொதுவாக குழந்தைகளின் ஊட்டச்சத்து குறைப்பாட்டை அவர்களின் கையில் நடுப்பகுதியின் மேல் சுற்றளவு -எம்.யு.ஏ.சி. (MUAC) அளவை கொண்டு கணக்கிடப்படுகிறது. நிலையான அளவு டேப் கொண்டு அளந்து இது பச்சை, மஞ்சள் சிவப்பு வகைப்பாட பிரிக்கப்படுகிறது. ஊட்டச்சத்து குறைப்பாட்டில், பச்சை நிற வகைப்பாடு என்பது எம்.யு.ஏ.சி. அளவு 12.5 செ.மீ. - 26 செ.மீ.க்கு இடைப்பட்டதாக இருக்கும். மஞ்சள் நிற வகைப்பாட்டில் 12.5 செ.மீ. - 11.5 செ.மீக்கு இடையிலும்; சிவப்பு நிற வகைப்பாட்டில் எம்.யு.ஏ.சி. அளவு 11.5 செ.மீ.க்கு குறைவாக இருக்கும்; இது கடும் ஊட்டச்சத்து குறைபாட்டையும், அவசர மருத்துவ பாதுகாப்பின் அவசியத்தையும் வெளிப்படுத்துவதாகும்.
பூர்ணிமாவின் குழந்தையுடைய கையின் நடுப்பகுதியை அளவிட்ட அங்கன்வாடி ஊழியர்கள், கோரங்கோவின் உடல்நிலை அபாயகட்டத்தில் இருப்பதாகக்கூறி, பொகாரோவில் உள்ள எம்.டி.சி. மையத்திற்கு அழைத்துச் செல்ல பரிந்துரை செய்தனர். பொகாரோவில் உள்ள எம்.டி.சி. மையம் 20 படுக்கைகளை கொண்டது; ஆனால் இந்தியா ஸ்பெண்ட் பார்வையிட்டபோது கோரங்கோ மட்டுமே நோயாளியாக சேர்க்கப்பட்டிருந்தது. எனினும், ஊட்டச்சத்து குறைபாடு குறைவாக உள்ளது என்பது இதன் பொருளல்ல.
எம்.சி.சி. மையத்திற்கு வரும் ஊட்டச்சத்து குறைபாடுள்ள குழந்தைகளின் பல பெற்றோர்களுக்கு அதுதான் கடைசி முடிவாக உள்ளது; ஏனெனில், குடும்பங்கள் தங்களுடைய தினசரி ஊதியத்தை இழக்க அஞ்சுகின்றன. பொகாரோ சுகாதார மையத்திற்கு பூர்ணிமா தேவி வருவதற்கு, ஜார்க்கண்ட்- மேற்கு வங்க எல்லையில் உள்ள தனது கிராமத்தில் இருந்து 10 கி.மீ. தொலைவு பயணம் செய்ய வேண்டியிருந்தது. மற்றவர்கள் மாவட்ட தலைமையகத்தை அடைய 40 கி.மீ.க்கு பயணம் செய்ய வேண்டும். “ஆகஸ்ட் மாதம் விதைப்பு பருவம் என்பதால் விவசாய தொழிலாளர்கள் தேவை அதிகமாக இருக்கும்” என்று, பொகாரோ எம்.டி.சி. பணியாளர் நிஷா சிங் தெரிவித்தார். “தங்கள் குழந்தைக்கு ஊட்டச்சத்து குறைபாடு இருப்பினும், இங்கு வருவதற்காக ஒருநாள் கூலியை விட்டுக்கொடுக்க பெற்றோர் விரும்புவதில்லை. அவர்கள், அருகில் உள்ள அங்கன்வாடி மையங்களுக்கு குழந்தையை கொண்டு செல்வர்; அல்லது வீட்டிலேயே சிகிச்சை அளித்து தோல்வி காண்பார்கள்” என்றார்.
கிழக்கு பொகரோ மாவட்டம் சந்தங்கிரி ஒன்றியம் தெக்கோரா கிராமத்தில் உள்ள அங்கன்வாடி தொழிலாளர் சாயா முகர்ஜி இந்தியா ஸ்பெண்டிடம் கூறுகையில் அங்கன்வாடி மையத்தில் தான் பணிபுரிந்த இரண்டரை ஆண்டுகளில், எம்டிசியில் குழந்தைகளை சேர்க்க தயங்கிய பல தாய்மார்களை கண்டதாக கூறினார். தனது பகுதியில் 3 குழந்தைகள் கடும் ஊட்டச்சத்து பற்றாக்குறையால் அவதிப்பட்ட நிலையில் ஒரு குழந்தை மட்டுமே எம்.டி.சி.யில் அனுமதிக்கப்பட்டிருந்ததாக அவர் தெரிவித்தார். "ஒருசில தாய்மார்கள் ஊட்டச்சத்து குறைபாடுகளை புரிந்து கொள்ளத்தவறிவிட்டார்கள், பலரும் வேலைகளை விட்டு வர முடியாது," என்றார் முகர்ஜி.
ஒரு சந்தர்ப்பத்தில், 25 வயதான கொஸாம்தேவி தனது ஒன்பது மாத குழந்தையை எம்.டி.சி.க்கு கொண்டு வந்தார். அக்குழந்தை ஒருமுறை மட்டுமே உற்சாகமடைந்தது. "குழந்தையின் நிலை பற்றி முன்பே நாங்கள் எச்சரிக்கை செய்தோம்; ஆனால் அவர் தனது கிராமத்தில் இருந்து 50 கி.மீ. தொலைவில் உள்ள எம்.டி.சி.க்கு வரவில்லை; போக்குவரத்திற்கு அவரிடம் பணம் இல்லை" என்று முகர்ஜி தெரிவித்தார்.
கொஸும் தேவி (நடுவில் இருப்பவர்) தனது கணவர் (இடது) மற்றும் ஒன்பது மாத ஊட்டச்சத்து குறைபாடுள்ள குழந்தையுடன். அருகில், பொகாரோ ஊட்டச்சத்து சிகிச்சை மையத்திற்கு அவர்களை அழைத்து வந்த அங்கன்வாடி பணியாளர்.
"தாய்மார்கள் தினந்தோறும் கூலி வேலைக்கு செல்வதானால், ஒவ்வொரு ரூபாயும் அவர்கள் கணக்கிடுகிறார்கள்," பூர்ணிமா கூறினார். "எம்.டி.சி. சார்பில் குழந்தையின் உதவியாளருக்கு நாளொன்றுக்கு 100 ரூபாய் இழப்பீடு தரப்படுகிறது; ஆனால், உணவுக்கு மட்டும் தான் போதுமானது. வேலைக்கு செல்லாமல் குழந்தையை பார்த்து கொண்டிருந்தால், அவர்கள் குடும்பத்தில் மற்றவர்கள் எப்படி வாழ்வார்கள்?” என்று அவர் கேட்டார்.
பூர்ணிமாவின் இக்கட்டான சூழ்நிலைக்கு வறுமை என்பது அடிப்படை காரணம். ஊட்டச்சத்து குறைபாட்டைத் தவிர்ப்பதற்காக, பாலூட்டும் ஒரு தாய் காய்கறிகள், நார் மற்றும் புரதம் நிறைந்த உணவுகளை சாப்பிட வேண்டும். ஆனால், மிஞ்சிய உணவுகளை தான் பூர்ணிமா சாப்பிடுகிறார். ”மற்ற பெண்களை போல தான் நானும் வீட்டில் கடைசியாக உணவு சாப்பிடுகிறேன். ஒரு நாளை இரண்டு முறை வேகவைத்த அரிசி, கொஞ்சம் பருப்பு என கிடைப்பதை சாப்பிடுகிறேன்” என்று இந்தியா ஸ்பெண்டிடம் பூர்ணிமா தெரிவித்தார். அவருக்கு ஊட்டம் நிறைந்த உணவு தேவை என்பதை குடும்பத்தினரும் அறிவார்கள்; எனினும் உணவை அதிகம் தர முடியாது. தண்ணீர் பிடிப்பது, குடும்பத்தில் உள்ள ஏழு பேருக்கு சமைப்பது மற்றும் அவர்களின் துணிகளை துவைப்பது என்று, பூர்ணிமாவின் தினசரி வாழ்க்கை நகர்கிறது; சுய பாதுகாப்பு குறித்து அவர் அக்கறை எடுத்துக் கொள்ள முடிவதில்லை.
ஜார்கண்ட் மாநிலத்தில் வறுமைக் கோட்டுக்கு கீழே உள்ள பெரும்பான்மையான பெண்களின் கதையும் பூர்ணிமாவை போன்றது தான். இங்குள்ள பல செவிலியர் தாய்மார்கள், ஒருநாளைக்கு இரண்டு வேளை உணவே உண்டு ஊட்டச்சத்து குறைவோடு உள்ளனர்; ஊட்டக்குறைபாடு உள்ள குழந்தைகள் பிறக்க இது வழிவகுக்கிறது.
கல்வியின்மை மற்றும் ஊட்டச்சத்து குறைபாடு ஆகியவற்றுக்கு இடையே நெருக்கமான இணைப்பு உள்ளது. இந்தியாவின் 2011 மக்கள் தொகை கணக்கெடுப்புபடி, ஜார்க்கண்டின் மக்கள்தொகையில் 76% கிராமப்புறங்களில் வாழ்கின்றனர்; இதில் இந்திய சராசரி 31% ஆகும். இந்திய கிராமப்புற பெண்களின் கல்வி விகிதம் 62% என்பதுடன் ஒப்பிடும்போது, ஜார்கண்ட் மாநில கிராமப்புற பெண்களில் 46.62% கல்வி பெற்றுள்ளனர். ஜார்க்கண்ட் கிராமப்புறங்களில் 15-49 வயதுடைய பெண்களில் 67.3%; ஆறு முதல் 59 வயதுடைய பெண்களில் 71.5% பேர் ரத்தசோகையால் பாதிக்கப்பட்டுள்ளனர். இதில் தேசிய சராசரி முறையே 53.1% மற்றும் 58.6% என்று உள்ளதாக என்.எப்.எச்.எஸ். புள்ளி விவரங்கள் தெரிவிக்கின்றன.
பல பெண்கள் 18 வயதிற்கு முன்பே திருமணம் செய்து கொண்டனர், 14 வயதிற்கு உட்பட்டவர்களாகவும், அவர்களுக்குக் கல்வி கற்றுக்கொடுப்பது குறைவாகவும் உள்ளது. ஜார்கண்ட் மாநிலத்தில் 37.9% பெண்கள் திருமணத்திற்கும் குறைவான வயதுடையவர். இது நாட்டின் மூன்றாவது உயர்ந்த விகிதமென என்.எப்.எச்.எஸ். தரவுகளை கொண்ட எமது பகுப்பாய்வு காட்டுகிறது. "எந்த வயதினரும் தங்கள் வயது என்ன என்று கேட்கும்போது 25 இருக்கும் என்று பதில் அளிக்கின்றனர்" என்று ஒரு அங்கன்வாடி ஊழியர் தெரிவித்தார். "குடும்ப உறுப்பினர்கள் தங்கள் பிறந்த தேதி பற்றி தெரியாது. ஆதார் அட்டையில் (மத்திய அரசின் தனித்துவ அடையாளம் காணும் திட்டம்) பதிவு செய்யும்போது, தாய்மார்கள் பலர் தங்கள் வயதை 18 என்றே குறிப்பிட்டுள்ளனர். 14 வயதான பெண்களை பள்ளியில் இருந்து நிறுத்தி திருமணம் செய்து வைக்கப்பட்டிருப்பதை தனிப்பட்ட முறையில் நான் கண்டேன்”. தனக்கு 25 வயது என்றும் ஆனால் பார்ப்பதற்கு இன்னும் இளையவராக தெரிவதாக, பூர்ணிமா தேவி கூட தெரிவித்தார்.
சுகாதார குறைபாடு நிலைமைகள் நோய்களின் பரவலுக்கு காரணமாகின்றன; இது ஊட்டச்சத்துக் குறைபாட்டின் மற்றொரு முக்கிய காரணம். ஜார்க்கண்ட் கிராமங்களில் குடிநீர் என்பது சுத்தமற்றது; பெரும்பாலும் பாசி நிறைந்த குளங்களில் இருந்து குடிநீர் பெறப்படுகிறது.
ஊழியர்கள், ஆதார வளங்களால் ஊட்டச்சத்து குறைபாட்டுக்கு எதிரான போராட்டத்தில் முன்னிலை வகிக்கும் ஜார்கண்ட் அங்கன்வாடி மையங்கள்
கடந்த 1990ஆம் ஆண்டுகளில் இருந்து ஊட்டச்சத்து குறைபாடு தொடர்பான பாதிப்புகள் இந்தியாவில் குறைந்து வருகிறது. 2016ஆம் ஆண்டில் இந்தியாவின் மொத்த நோய் பாதிப்பில் ஊட்டச்சத்து குறைப்பாட்டின் பங்கு 15% என்றளவில் இருந்தது என, “இந்தியா: ஹெல்த் ஆப் தி நேஷன்’ஸ் ஸ்டேட்டஸ்” இந்தியாவின் மாநில அளவிலான நோய்கள் சுமை குறித்த முன்முயற்சியின் அறிக்கையில் தெரிவிக்கப்பட்டுள்ளது.
தேசிய அளவில் பத்து ஆண்டுகளுக்கு முன் ஒப்பிடும் போது, 2015-16ஆம் ஆண்டில் குழந்தைகள் ஊட்டச்சத்து குறைபாடு 9.6% புள்ளி குறைந்துள்ளது. ஆனால் ஜார்கண்டின் முன்னேற்ற விகிதம், 4.5% என என்.எப்.எச்.எஸ். தரவின் எங்கள் பகுப்பாய்வு காட்டுகிறது.
Source: National Family Health Survey 4 (2015-16)
கடந்த 2017, நவம்பர் 21ல் ஜார்கண்ட் முதலமைச்சர் ரகுபார் தாஸ் ஓர் அறிவிப்பை வெளியிட்டார். அதன்படி, ஊட்டச்சத்து குறைபாட்டை குறைக்கும் வகையில், 2018ஆம் ஆண்டு ‘நிரோக் பால் வர்ஷ்’ ( ஆரோக்கிய குழந்தைக்கான ஆண்டு) என கடைபிடிக்கப்படும் என்று அறிவிக்கப்பட்டது. “அடுத்த மூன்று, நான்கு ஆண்டில் ஊட்டச்சத்து மிகுந்த மாநிலங்களில் முதல் 10 இடங்களுக்குள் வருவதே ஜார்க்கண்டில் இலக்கு” என்று தாஸ் தெரிவித்தார்.
எனினும், அந்த இலக்கை அடைய ஜார்க்கண்ட்டிற்கு ஒரு நீண்ட நெடிய பயணமாக உள்ளது. 2018 ஆகஸ்ட் 19ல், தலைநகர் ராஞ்சியில் உள்ள சர்தார் மருத்துவமனையில் ஒரு குழந்தை, தனியார் மருத்துவமனையில் மற்றொரு குழந்தை உயிரிழந்தது. ஒரு வாரத்திற்குள்ளாக ஆகஸ்ட் 24ஆம் தேதி, தாயால் கைவிடப்பட்ட ஒரு ஆண் குழந்தை, ராஞ்சி ராஜேந்திரா மருத்துவ அறிவியல் கழக மருத்துவமனையில் இறந்தது. இம்மூன்று குழந்தைகளுமே எடை குறைபாடு, ஊட்டச்சத்துயின்மையால் இறந்தன.
ஜார்கண்ட் மாநிலத்தில் ஊட்டச்சத்து குறைபாடுள்ள குழந்தைகளின் எண்ணிக்கை அதிகம் இருப்பது, ஊட்டச்சத்து திட்டங்களின் செயல்திறனை கேள்விக்குறியாக்குகிறது. மாநில சமூக நலத்துறையால் நடத்தப்படும் அங்கன்வாடி மையங்கள், பெரும்பாலான குழந்தைகளுக்கு அணுகல் இடமான ஐ.சி.டி.எஸ். போன்றவற்றில் போதிய ஊழியர், ஆதாரவளங்கள் இல்லாததுடன் போராட வேண்டியுள்ளது.
பெயர் வெளியிட விரும்பாத, பொகாரோ மாவட்ட அங்கன்வாடி மைய மேற்பார்வையாளர் இந்தியா ஸ்பெண்டிடம் கூறுகையில், பணியாளர் பற்றாக்குறை இதற்கான காரணம் என்றார். ”பொகாரோ மாவட்டத்தில் 324 அங்கன்வாடி மையங்கள் உள்ளன; ஆனால், எதிலும் முழுமையான வசதிகள் இல்லை” என மேற்பார்வையாளர் தெரிவித்தார். “ஒவ்வொரு அங்கன்வாடி ஊழியரும் குறைந்தது 35 மையங்களுக்கு பொறுப்பாக உள்ளார். ஒவ்வொன்றும் வெகுதூரத்தில் உள்ளது; அவற்றை சென்றடைய சாலை (பாதை) வசதியில்லை என்பதால், சேவை புரிவது கடினமாக உள்ளது” என்றார். மோசமான, வெளிச்சமற்ற பொகாரோ கிராமப்புற சாலைகள் நிலைமையை மேலும் மோசமாக்குகிறது. பொகாரோ எம்.டி.சி. வருவதற்கு 6 கி.மீட்டருக்கு மேல் நடந்து, இரண்டு பேருந்துகளை பிடிக்க வேண்டும் என்று, பூர்ணிமா தேவி தெரிவித்தார்.
"பொகரோவிலிருந்து தெக்கோரா கிராமத்திற்கு 22 கி.மீ. தொலைவில் காடுகள், சாலைகளில் நாங்கள் பயணம் செய்ய வேண்டும். கிராமங்களுக்கு இடையே சென்று வருவதற்குள் சோர்வு ஏற்பட்டுவிடுகிறது” என, சந்தன்கியரி ஒன்றிய அங்கன்வாடி மேற்பார்வையாளர் ரூபா குமாரி தெரிவித்தார். “ஆனால், எங்களுக்கு இது கொஞ்சம் தான்; நிறைய குழந்தைகள் அவசர உதவி தேவையோடு இருக்கிறார்கள்; அவர்களுக்கு உதவ நாங்கள் விரும்புகிறோம்” என்றார் ரூபா.
கடந்த இரண்டு ஆண்டுகளாக மாநில அரசு பயணப்படியை வழங்காத நிலையில் மேற்பார்வையாளர்கள் தங்களின் சொந்த பணத்தில் கிராமங்களுக்கு சென்று வருவதாக, ஒரு மேற்பார்வையாளர் தெரிவித்தார். எம்.டி.சி., அல்லது மாவட்ட தலைமையகத்தில் குழந்தைகள் அல்லது மேற்பார்வையாளர்களுக்கு உதவுவதற்காக வாகனங்கள் இல்லை.
சிக்கலான நிலையில் எம்.டி.சி.யில் விடப்படும் குழந்தைகள், ஊட்டச்சத்து குறைபாடு உள்ள தாய்மார்கள், குழந்தைகள் போதிய ஊட்டம் பெறச் செய்தல் என்று அங்கன்வாடி ஊழியர்களுக்கு பணிச்சுமை அதிகளவில் உள்ளது. ஒரு ஊட்டச்சத்து குறைபாடுள்ள குழந்தை மருந்திற்காக குறைந்தபட்சம் 15 நாட்களுக்கு எம்.டி.சி.யில் மருந்து மற்றும் கண்காணிப்புக்காக அனுமதிக்கப்பட வேண்டும்; ஆனால் பெரும்பாலான பெற்றோர்கள் இரண்டு நாட்களுக்கு மேல் தங்க மறுக்கிறார்கள்; அவர்கள் தினசரி சம்பளம் இழந்துவிடும் என்ற அச்சமே காரணம். அங்கன்வாடி ஊழியர்களின் பொறுப்புகள், 15 நாட்களுக்கு தங்குவதற்கு குடும்பத்தினருக்கு ஆலோசனை வழங்குவதும் அடங்கும். இத்தகைய ஆலோசனைக்கு வழங்கும் ஊழியர்களுக்கு கடும் பற்றாக்குறை உள்ளதன் விளைவுகள், அவர்கள் முழு 15 நாள் சிகிச்சைக்கு செல்லவில்லை என்றால் ஊட்டச்சத்து நிறைந்த குழந்தைகள் உருவாவதை அதிகரிக்கிறது.
ஜார்க்கண்ட் மாநிலத்தில் தேசிய ஊரக சுகாதார திட்டத்தை செயல்படுத்தும் மத்திய சுகாதார மற்றும் குடும்ப நலத்துறை இயக்குனர் கிருபானந்த் ஜா, ஊட்டச்சத்து குறைப்பதற்கான நடவடிக்கைகளை துரிதப்படுத்துவதாக கூறுகிறார். “ஜார்க்கண்ட் மாநிலத்தில் 88 சதவீத குழந்தைகளுக்கு சிகிச்சை தரப்பட்டுள்ளது; 75 சதவீதம் வாய்வழியே உப்பு கரைசல் தரப்பட்டுள்ளது” என்று ஜா தெரிவித்தார்.
மாநிலத்தின் குழந்தைகளுக்கான ஊட்டச்சத்து நெருக்கடியை சமாளிக்கும் வகையில் மருந்து வினியோகம் மீதான கவனம் போதுமானதாக இல்லை. ஐ.சி.டி.எஸ் மற்றும் அங்கன்வாடி மையங்களை நன்கு பராமரிப்பது மற்றும் குழந்தை ஊட்டச்சத்து குறைபாடுகளை அங்கன்வாடி பணியாளர்கள் சமாளிப்பது மிகவும் திறமையான அணுகுமுறையாக இருக்க முடியும் என்று இந்த சிறப்பு திட்டம் காட்டுகிறது.
பொகரோவின் ஊட்டச்சத்து மேலாண்மை சிறப்பு திட்டம் ஜார்கண்டிற்கு வழி காட்டுகிறது
பொகாரோ மாவட்டத்தின் சந்தன்கியாரி மற்றும் சாஸ் ஒன்றியங்களில், 2017 ஜனவரி- செப்டம்பர் இடையே ஒன்பது மாதங்கள் செயல்படுத்தப்பட்ட ‘சமுதாய அடிப்படையிலான தீவிர ஊட்டச்சத்து மேலாண்மை’ (CMAM) சிறப்பு திட்டம், குழந்தைகளின் ஊட்டச்சத்து குறைபாடுகளை குறைக்க பெரிதும் உதவியது. ஜார்க்கண்ட் மாநில ஊட்டச்சத்து இயக்கம், அரசுசாரா அமைப்பான வேர்ல்ட் விஷன் இந்தியா (WV India) உடன் சேர்ந்து இந்தியா முழுவதும் சுகாதார வசதிகளை மேம்படுத்துதல், ஆதரவு மேற்பார்வை மற்றும் திறனை வளர்ப்பதில் அனுபவத்தை கொண்டு, இத்திட்டத்தை செயல்படுத்தியது.
இத்திட்டத்தில் வீடுவீடாக சென்று குழந்தைகள் கண்காணிக்கப்பட்டனர்; அவர்களது கையின் நடுப்பகுதி சுற்றளவு அளவிடப்பட்டது. டபிள்யூ.வி. இந்தியா அங்கன்வாடி ஊழியர்களுக்கு பயிற்சி அளித்ததோடு தன்னார்வலர்களை கொண்டு பயிற்சியை கண்காணித்தது. இந்த திட்டம், மஞ்சள் மற்றும் சிவப்பு நிற வகைப்பாடு அடையாளம் கொண்ட குழந்தைகளுக்கு, அதாவது முறையே மிதமான ஊட்டச்சத்து பற்றாக்குறை நிலை மற்றும் தீவிர ஊட்டச்சத்து பற்றாக்குறை நிலை என்ற பிரிவில் சிகிச்சை அளிப்பதை மையமாகக் கொண்டது.
இதன் முடிவுகள், மஞ்சள் நிற வகைப்பாட்டில் இருந்த 158 குழந்தைகளில் 96 பேர் (61%) ஊட்டச்சத்து குறைபாட்டில் இருந்து மீண்டனர். சிவப்பு நிற வகைப்பாடு குழந்தைகள் உடனடியாக எம்.டி.சி.களுக்கு அனுப்பப்பட்டனர்.
"டபிள்யூ.வி. இந்தியாவின் ஈடுபாட்டிற்கு முன்னர் ஊட்டச்சத்து குறைபாடுகளின் எண்ணிக்கை குறைவாக இருந்தது" என, அதன் தொழில்நுட்ப வல்லுனரான கிரானாபுல் செல்வி இந்தியா ஸ்பெண்டிடம் தெரிவித்தார். "ஆதார வளங்களும், நேரமும் இல்லாததால், களத்தில் உள்ள அரசு ஊழியர்கள் ஊட்டச்சத்துள்ள குழந்தைகளை அடையாளம் காண முடியவில்லை. உண்மை கள நிலவரம் வேறு மாதிரியாக இருப்பினும், மூத்த அதிகாரிகள் நம்பிக்கையூட்டும் வகையில் சித்தரித்தனர்” என்றார்.
டபிள்யு.வி. இந்தியாவின் உறுதியான நிறுவன ஆதரவு, மருந்து வழங்கலை உறுதி செய்தது; சத்தான உணவு, குழந்தைகளின் துல்லியமான நிலை குறித்து ஆய்வறிக்கை தந்தது என செல்வி கூறினார். ஐ.சி.டி.எஸ். செயலாக்கத்திற்கான மாநில அரசுடன் இந்த குறுகிய கால ஒத்துழைப்பு சாதகமான முடிவுகளை வழங்கியது என அவர் மேலும் கூறினார்.
பொகாரோ மாவட்டத்தில் உள்ள அங்கன்வாடி மையம் ஒன்றின் சுவற்றில் ஊட்டச்சத்து மிகுந்த உணவு குறித்து மக்களுக்கு விழிப்புணர்வு ஏற்படுத்தும் விளம்பரம் இடம் பெற்றுள்ளது.
சி.எம்.ஏ.எம். திட்டம், பிரச்சனைகளை ஒரு வரம்புக்குள் நிர்வகிக்க உதவியது என்று மாநில சமூகநல துறை தலைவர் சுமன் குப்தா, பொகாராவில் இந்தியா ஸ்பெண்டிடம் தெரிவித்தார். "இது ஊட்டச்சத்து குறைபாட்டின் மோசமான சூழ்நிலையை புரிந்துகொள்ள உதவியது; இதன்மூலம் குழந்தைகள் உடனடியாக பராமரிக்கப்பட்டனர். அரசால் வளங்களை நன்கு நிர்வகிக்க முடிந்தது” என்று குப்தா தெரிவித்தார்.
"தாய்மார்களுடன் தொடர்பு கொள்வதற்கான வழிகளை வேர்ல்ட் விஷன் கற்பிப்பதன் மூலம் எங்கள் தொழில்முறை திறன்களை அதிகரிக்கிறது. நாங்கள் தாய்மார்களிடம் சுகாதார மற்றும் சுய பராமரிப்பு கவனத்தை கொஞ்சம் கொஞ்சமாக செலுத்த முடியும். அதுவே முன்னேற்றம் தான், "என்கிறார் ஒரு அங்கன்வாடி பணியாளர்.
(இந்த கட்டுரை குழந்தை சுகாதார, கல்வி மற்றும் குழந்தை பாதுகாப்பு குறித்த டபிள்யு.வி.ஐ. - எல்.டி.வி.(WVI- LDV) உடன் இணைந்த ஒரு பகுதியாக உள்ளது.)
உங்களின் கருத்துகளை வரவேற்கிறோம். கருத்துகளை respond@indiaspend.org. என்ற முகவரிக்கு அனுப்பலாம். மொழி, இலக்கணம் கருதி அவற்றை திருத்தும் உரிமை எங்களுக்கு உண்டு.
